Vertigo is a distressing and fearful symptom, one which provokes anxiety in the clinician also. The patient is fearful because they have lost their very equilibrium, shaken by the starkness of their distress. The time-pressured clinician is fearful as how to best expedite the case safely. In the back of every clinician’s mind is the nagging fear that this vertigo is the presenting feature of a life-threatening condition — a cerebellar stroke or a space occupying lesion.
How to perform a succinct clinical assessment that rules out serious pathology and provide acute symptom relief?
RED FLAGS ⇒ diffusion-weighted MRI (with MRA) is 83% sensitive
- focal neurological deficit
- total (ipsilateral) hearing loss
- inability to walk (or sit upright) without support
- direction-changing nystagmus
Vertigo is the illusion of movement, most commonly experienced as a spinning sensation, arising from a pathological imbalance in the peripheral or central vestibular system. About 0.7 – 3% of those with isolated vertigo have cerebellar infarction, which has a mortality up to 40%. CT scan is only 26% sensitive for acute stroke (cf. haemorrhagic stroke in which CT or MRI are equally useful), whereas physical signs are present in the majority of patients with cerebellar infarction.
Differentiate cerebellar infarction from the 4 most common vertigo syndromes:
- Benign Paroxysmal Positional Vertigo (BPPV)
- Meniere’s Disease
- Migrainous Vertigo
- Vestibular Neuritis
What does the patient mean by “dizzy”, “off balance”, or “light-headed”?
Most patients will report the classical rotational vertigo, but approximately 17% will not — these patients may report episodic imbalance or dizziness that is made worse with head movement.
Benign Paroxysmal Positional Vertigo (BPPV)
- brief episodes (< 1 minute) of intense vertigo, precipitated by a change in position — i.e. patients are well until a head movement, usually vertical, precipitates the paroxysm of symptoms
- usually idiopathic — otolith usually in posterior semi-circular canal → diagnosed by torsional nystagmus on Dix-Hallpike test
- only 10% follow a bout of vestibular neuritis
- only 20% follow episode of head trauma
[BPPV is the most common condition you will see, and Half Somersault Canalith Repositioning is the most practical self-treatment available. The other manoeuvre is the Epley, which starts off like a Dix-Hallpike. Lateral or horizontal canal BPPV can be managed with the Lempert manoeuvre.]
Meniere’s Disease (endolymphatic hydrops)
- suspect if simultaneous vertigo and cochlear complaints
- hearing loss (audiology may be normal between episodes)
- tinnitus
- aural fullness
- episodes usually last a few hours, although they can range from 20 minutes to a few days — if the patient has not had previous episodes, labyrinthitis (vestibular neuritis) should be suspected instead
[In general, vertigo with hearing loss, unless it is with total ipsilateral deafness, indicates a peripheral disorder.]
Migrainous Vertigo
- can be elusive — half of patients present without headache
- strict diagnostic criteria have been proposed
- recurrent episodes of vertigo
- formal migraine diagnosis (IHS criteria)
- migraine symptom during attack (headache, photophobia, aura)
- exclusion of other causes
[Cerebellar infarction is not expected to present with migraine-associated symptoms, so most patients with criteria for migrainous vertigo and a normal neurological examination can be treated for their migraine process without further work-up.]
Vestibular Neuritis
- acute vestibular syndrome, caused by decreased vestibular tone on one side (? viral aetiology)
- characteristic findings on history and ocular examination
- gradual onset — symptoms peak during first day and begin to improve within a few days (although full recovery takes weeks to months)
- associated vertigo is persistent and ongoing, although positional exacerbation is also characteristic, as any head movement amplifies the disparity in bilateral vestibular tone
- associated autonomous symptoms of nausea and vomiting are prominent
- general neurological examination, including limb coordination, is normal
- although some mild incoordination is suspected, the patient should retain the ability to ambulate
- nystagmus is unidirectional (regardless of where the patient looks the direction of nystagmus will not change) and is attenuated when looking away from the hypoactive ear (Alexander’s Law)
[Unidirectional nystagmus can occur in 46% of cerebellar infarction.]
They are the four big differentials of vertigo, apart from cerebellar infarction.
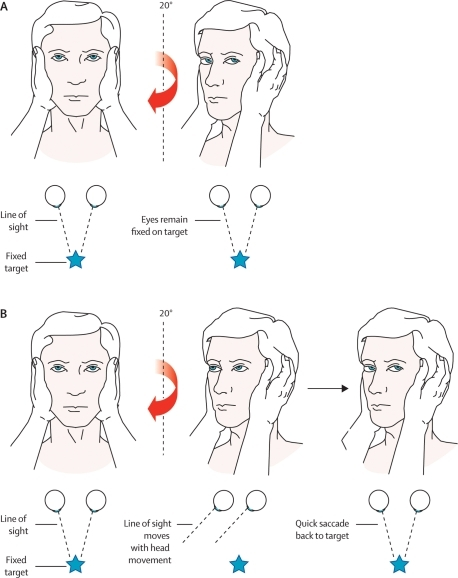
VOR – HEAD IMPULSE (THRUST) TEST

{kind=link}
Cerebellar Infarction
- approximately 2-3% of acute strokes, from either of
- superior cerebellar artery (SCA)
- anterior inferior cerebellar artery (AICA)
- posterior cerebellar artery (PICA)
[Large cerebellar infarcts produce symptoms and signs localising to the brainstem, such as diplopia, dysarthria, limb ataxia, dysphagia, and weakness or numbness.]
Approximately 10% of patients with cerebellar infarction can present with isolated vertigo, that is vertigo with no localising findings on motor, sensory, reflex, cranial nerve, or limb coordination examination — most of these (96%) are infarcts of the medial branch of the PICA.
⇓
These are the patients that are most often misdiagnosed, often with consequent disability → look for other pointers suggestive of stroke:
- severe ataxia (classically considered a sign of central vertigo) — inability to walk without support
- direction-changing (multidirectional or gaze-evoked) nystagmus — avoid extreme lateral strain which can produce end-point nystagmus, a normal finding that reflects only muscle fatigue
[These two signs are commonly present even when no other findings of brainstem ischaemia are present — at least one of these two signs is seen in 84% of patients with cerebellar infarction and isolated vertigo.]
. . .
This has been redacted from the review article by Nelson and Virre published in the Western Journal of Emergency Medicine, 2009 (see below for link).
Reference
- Nelson JA and Viirre E. The Clinical Differentiation of Cerebellar Infarction from Common Vertigo Syndromes. West J Emerg Med. 2009 Nov; 10(4): 273–277.
Further Reading
- Head Thrust: Differential Diagnosis for Vertigo. Vertigo Differentiation
- Abnormal Head Impulse Test – YouTube video (note: a “negative” test is abnormal)
- Taking a ‘Dizzy’ History – The Doctor
- Kattah JC, Talkad AV, Wang DZ, Hsieh Y-H, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009 Nov; 40(11): 3504–3510.
- Tarnutzer AA, Berkowitz AL, Robinson KA, Yu-Hsiang Hsieh, Newman-Toker DE. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ June 14, 2011 vol. 183 no. 9.
Featured Image
- James Stewart and Kim Novak in ‘Vertigo’. [Image: The Hitchcock Zone]